Two research teams participate in this consortium in a wide variety of activities and tasks. Therefore, the proper management of such objectives and tasks becomes crucial to maximize the positive results of this project. Thus, the following coordination plan has been designed to ensure successful collaboration:
- The project coordinator will organize meetings every two months. The meeting agenda will be agreed between the principal investigators (PI) of all subprojects. The agenda will include, at least, the following items: Approval of the minutes of the last meeting, Analysis of progress, Discussion of current issues, Planning of future actions and Updating of the expected risks.
- The execution and development of the project will be carried out by periodically writing technical reports, which will be distributed to all researchers.
- Face-to-face meetings are expected to take place twice a year (provided safe sanitary conditions are met), once organized and held by the members of a subproject and vice versa. All project members will be informed about the progress made. In recent years, the research groups of MINERVAS project have worked together and have successfully achieved results in the context of the aforementioned projects, with the following notable results: ● UJA-UOVI: Development of efficient musical accompaniment systems for mobile devices with the publications ([Alo17a] [Alo17b] [Cab18] [Cab19] [Muñ19] [Muñ20a]), Parallel source separation system for heart and lung sounds ([Muñ20b]) and a software license (ReMAS).
Background
Heart and lung diseases are one of the main causes of death in the world and, currently, the latter have increased exponentially due to the respiratory complications that the COVID-19 virus is generating. According to the World Health Organization (WHO):
- An estimated 17.5 million deaths from cardiovascular diseases in 2012 (30% of the total deaths registered in the world) and 23.6 million deaths from the same type of diseases have been predicted by 2030 [OMSa].
- It has been estimated that hundreds of millions of people suffer the consequences of chronic respiratory diseases (CKD) every day, of which approximately 235 million suffer from asthma, 64 million suffer from chronic obstructive pulmonary disease (COPD) and the rest from other CKD that are often undiagnosed. Specifically, almost 400,000 deaths from asthma were registered in 2004, especially in the elderly and child population as they are the most vulnerable sectors, mainly in countries with weak health systems [OMSb]. Approximately, 7% of the world population is suffering chronic respiratory diseases from 1990 to 2017 according to data from The Lancet [GRDC] as shown in Figure 1.
 Figure 1. All-age chronic respiratory disease prevalence by country in 1990 and 2017 [GRDC].
Figure 1. All-age chronic respiratory disease prevalence by country in 1990 and 2017 [GRDC].In addition to the fact that the suffering of these heart and respiratory diseases reduces the well-being and life-quality of citizens, the medical treatment that must be applied is increasing the costs of the health systems due to the multiple visits to medical centers and the large number of citizens who suffer from them. Consequently, it is interesting to investigate new techniques that allow monitoring and obtaining fast, reliable and individualized biomedical information to establish personalized medicine as a strategy for sustainability and efficiency in health systems. It is at this point where the use of the eHealth concept becomes interesting and necessary, trying to apply new techniques and tools derived from Information and Communication Technologies (ICT). The objective is to be able to attend, healthily and economically, an increasing fraction of the population using reliable, lower-cost and non-invasive techniques so that monitoring tasks are transferred step by step to the subject, which will significantly lower the costs. Thus, eHealth could be useful in the following scenarios:
● Retrieval of biomedical information related to the appearance of cardiac or respiratory risk factors [Cat17] [Ses18]:
i) estimation of heart rate (HR);
ii) detection of heart murmurs (HM);
iii) estimation of heart rate variability (HRV);
iv) estimation of respiratory rate (RR);
v) estimation of QT interval (QT, time from the start of the Q wave to the end of the T wave). addressed in a non-invasive way from the analysis of ECGs and cardiopulmonary sound signals to be applied to the continuous monitoring of the cardiac, respiratory and nervous activity of the subject. The development of strategies that combine the joint use of this information (HR, HM, HRV, RR and QT) could improve the reliability of diagnoses and minimize medical decision times.
● Retrieval of biomedical information related to the presence of alert situations applying robust, cheap, non-invasive and accessible techniques to citizens so that they can be performed individually from the analysis of lung sounds, such as coughing, wheezing, respiratory sounds and from the analysis of the limb I-lead ECG.In the field of HR estimation, most of the published works are based on ECG signals. In fact, ECG signal is the reference method for HR monitoring [Dia19]. However, even when using a wearable to get the limb I-lead ECG, it should be carried intentionally, avoiding the possibility of monitoring the ECG continuously in real time (the use of a holter-ecg is not real time). The cardiac auscultation process, phonocardiography (PCG), performed using a stethoscope or microphone normally placed on the subject's chest, allows listening to the sounds emitted by the heart where each cardiac cycle consists of two main sounds: S1 (systole) followed by S2 (diastole) [Chen15]. In that case, the HR estimate can be measured as the distance between two S1 sounds in a similar way as occurs in the succession of two R peaks in an ECG signal [Dia19]. In general, HR estimation methods can be divided into two broad categories [Kumar06]: methods that use a reference ECG signal and methods that do not use an ECG signal but sound signals [Kumar06] [Ari08] [Papadaniil14] [Dia19]. This research project is focused on the latter methods. Thus, Kumar and others [Kumar06] used wavelet decomposition; Ari et al [Ari08] presented a low pass filtering method where the filtered energy peaks were classified; in [Papadaniil14], Ensemble Empirical Mode Decomposition (EEMD) was applied; and recently, Dia and others [Dia19] have proposed a system based on NMF from cardiac sound signals applying the source-filter model with promising results.
When using a wearable to get the limb I-lead ECG, the signal is strongly related, among others, to sudden deaths as a consequence of fatal ventricular arrhythmias due to aberrant QT intervals [El-sherif20]. Improper use of medicaments used against COVID-19 is a recent and clear example [Jankelson20]. Regarding the measurement of the QT interval, there are also prior studies like [Haixia19] that are based on the previous estimation of the QRS complex [Rahul20] and the T wave from ECG. However, given that the detection of the T wave and the location of its end represents some difficulty as it can be confused with the isoelectric line or when there are alterations in morphology [Immanuel16], its extraction requires a particular analysis and treatment. In addition, it is also necessary to estimate the corrected QT interval in order to refer to the duration of the QT interval at 60 ppm. This project considers new AI-based techniques for classification and knowledge acquisition systems for the QT interval estimation from the limb I-lead ECGs, which is the lead that can be obtained from a typical wearable device.
Although auscultation is still the most widely used method applied to a subject who goes to a health center for the first time to assess the state of his heart, this method is highly subjective because it is conditioned to the skill, experience and training of each doctor in the type of sounds he/she is hearing. The appearance of HM must be detected, these murmurs are indicators of cardiac anomalies (mainly of the heart valves) and act as interference for a correct estimation of HRV by being temporarily separated from normal heart sounds in an interval less than 30 ms, which makes it difficult to detect through sound analysis. Many works published in this area have been based on ECG signals. However, in this project we will focus on the detection of HM using sound signal analysis without using ECG information for its detection (only for evaluation if necessary) because it could be implemented in mobile devices. In the existing literature in this line of research, most systems for detecting HM are usually composed of three stages [Yuenyong11]: segmentation of heart sounds S1 and S2, extraction of characteristics and classification [Wei19]. A support vector machine (SVM)-based classifier was used to discriminate normal and abnormal heart sounds using subspace analysis [Ghaderi11]. Jusak et al [Jusak16] demonstrated that EEMD provides fewer modes to generate the extracted SCs compared to CEEMD (complete EEMD). Other authors addressed the elimination of ambient noise mixed acoustically with cardiac sound signals [Naseri13]. Other NMF-based methods have been used in biomedical signal separation tasks with promising results [Muñ20b]. Thus, Shah and others [Shah14] investigated the potential of NMF in the separation of HM. Recently, Wei and others [Wei19] developed a cardiac sound segmentation system using the standard deviation of the Short Time Fourier Transform (STFT) as a characteristic, together with an algorithm for generating HM characteristics based on clustering of systolic frames
HRV is a parameter that informs about the state of the activity of the autonomic nervous system and is used as an indicator in cardiovascular risk factors [Cat17] [Ses18]. In fact, HRV is increasingly being used to measure both the physical and mental health status of subjects: stress level, presence of chronic heart disease, speed of health recovery in critical illness, etc. Although most of the published work on HRV is based on ECG signals, lately the scientific community has focused its efforts on methods based on the analysis of sound signals [Li13] [ Kamran13] [Shah14] [Sharma14] [Yil14] [Chen15] [Sharma19] [Dia19]. Li et al [Li13] applied a cyclostationary envelope with peak detection based on energy thresholding. In [Sharma14], HRV was estimated with heart sounds applying binary search and Shannon energy where the medium frequency components were emphasized and the low intensity components were attenuated. In [Shah14], a hierarchical NMF decomposition was applied whereby HRV was determined from acoustically separated cardiac sound signals. Sharma et al. [Sharma19] proposed the Hilbert-Huang transform (HHT) to construct an instantaneous energy envelope applied to cardiac cycle segmentation using the K-means algorithm.
With respect to the RR estimation, it has been defined as one of the key parameters hours before a patient enters a critical condition, such as readmission to the intensive care unit (ICU), chronic heart failure or pneumonia as the body tries to maintain oxygen delivery to the tissues. Specifically, a RR below 6 breaths/min and a RR above 24 breaths/min more reliably predicts the mortality of a patient when compared with the information provided by HR or blood pressure [Liu19]. In fact, an RR higher than 27 breaths/minute was the most determining indicator in predicting the onset of cardiac arrest in hospital wards [Nam2016]. Although there is an accepted definition for a normal HR (60-100 beats/minute) in adults, a normal RR in an adult is set at 12-20 breaths/min [RCP15] [RCP17]. However, despite the medical importance of the RR parameter, nowadays it is still not possible to obtain it in a reliable, cheap and individualized way. According to the literature in this field, the most common methods for monitoring RR are the following [Nam2016a] [Liu19]: i) manual counting of chest wall movements (easy, non-invasive, imprecise and slow); ii) Spirometry (accurate, interference with natural breathing and difficulty in maintaining continuous monitoring); iii) Capnography (precise, easy, allows continuous monitoring, uncomfortable due to device contact); iv) Auscultation of breath sounds with a stethoscope (easy, non-invasive, imprecise). Based on research, in the last decade it has been shown that these counting methods tend to be unreliable [Hillman05] [Kellet11], with a multitude of acoustic and non-acoustic methods [Muthusamy19] appearing to estimate RR. In this project, we will focus on those methods based on the analysis of respiratory sound signals captured by microphones or stethoscopes, among which those based on the detection of the inspiration/expiration phases [Chuah04] [Kulkas09] [Palaniappan15], relative changes of the energy distribution in frequency [Nakano04], Shannon entropy [Yadollahi06] [Gomes18], adaptive filtering [Golabbakhsh05], bioacoustic analysis [Hult00] and spectral dynamic characteristics of the nasal air flow in the inspiration/expiration stages [Nam2016a].
Several studies have shown the relation between cough, dyspnea, wheezing and vital signs and the exacerbation of several chronic diseases such as asthma, Chronic Obstructive Pulmonary Disease (COPD), bronchiectasis, etc [Niimi2011] [Roversi2018] [Sumner2013] [Smith2006] [Frappé2012] [Burgel2013] [Doenges2020]. Asthma is the most common cause of cough, wheezes, and dyspnea in children and adults [Weinberger2007]. However, cough can occur with pertussis, cystic fibrosis, primary ciliary dyskinesia, airway abnormalities such as tracheomalacia and bronchomalacia, chronic purulent or suppurative bronchitis in young children, and habit-cough syndrome [Weinberger2007]. Asthma is a disease in which the airways narrow excessively in response to various stimuli in the presence of airway hyper-responsiveness and eosinophilic airway inflammation. In “classic asthma” (CA) variable airflow obstruction typically leads to symptoms such as monophonic or polyphonic wheezes [Ulukaya19], dyspnea and cough [Niimi2011]. In ‘variant asthma’ usually named ‘cough variant asthma’ (CVA) cough can be the sole presenting symptom. CVA remains one of the most typical causes of chronic cough worldwide [Niimi2011]. On the other hand, COPD is characterized by airway inflammation and progressive airflow obstruction, most commonly caused by cigarette smoking and indoor air pollution. Cough, shortness of breath and sputum production are the major symptoms of which patients complain, although the relative importance depends on the stage of disease [Smith2006]. Although prevalence rates vary across published literature, it is estimated that about 17–35% of patients with heart failure are affected by COPD [Roversi2018]. In the era of TICs applied to health (eHealth), some studies [Roversi2018][Sumner2013] highlight the importance of continuously measuring and monitoring patients’ symptoms. Grading shortness of breath may point physicians in the right direction when evaluating stable, smoking patients with heart failure, i.e. suspecting the presence of lung impairment and help uncovering COPD [Roversi2018]. In this sense, a careful medical assessment of symptoms is the first approach for making a correct diagnosis (although additional investigations such as spirometry are eventually required). Stable COPD patients cough much more by day than night and most of them seem to be sensitive to the time spent coughing, as in large surveys the presence of the symptom is very commonly reported. Objective cough counts provide new insights, and ultimately automated cough counting [You17] will provide new objective outcome measures in COPD [Smith2006]. In [Sumner2013], ambulatory objective monitoring provides novel insights into the determinants of cough in COPD, suggesting sputum production, smoking, and airway inflammation may be more important than sensitivity of the cough reflex. As chronic respiratory symptoms and the presence of expiratory flow limitation (EFL) are commonly reported in the elderly, chronic cough and the composite outcome "chronic cough or sputum" were significantly associated with the presence of EFL [Frappé2012], concluding that monitoring could be advocated in elderly subjects presenting with respiratory symptoms. Finally, some works encourage continuing monitoring symptoms to evaluate the exacerbations of asthma and COPD [Frappé2012] [Burgel2013] [Infante17] [Doenges2020]. In [Burgel2013], it is stated that objective cough frequency monitoring of COPD patients could represent an interesting novel approach for complementing current methods of cough measurement that include subjective assessment of cough via questionnaires, symptoms diaries, visual analog scale, and self-counting of cough via the push-button method. Infante et al. [Infante17] reported that the analysis of cough sounds seemed to perform just as reliable as wheeze or crackle analysis for diagnostic prediction, concluding that cough sounds have value as a rapid and simple pulmonary analysis tool. In [Doenges2020], it is stated that patients with nocturnal symptoms like wheezing and cough often suffer from lower sleep quality and impaired daytime performance. The lack of an appropriate method for standardized and objective monitoring of respiratory symptoms leads to difficulties in asthma management. They proposed a new method for automated wheeze and cough detection during sleep and to assess the actual level of asthma control by the Asthma Control Test (ACT), classifying asthma as “controlled”, “partially controlled” or “uncontrolled” within the last 4 weeks.
The main methods for detecting cough are based on Neural Networks (NN) [Barry06] [Bales20], Empirical Mode Decomposition (EMD) [Ferdousi15], Hidden Markov Models (HMM) [Matos07], Principal Component Analysis (PCA) [Abaza09a], characteristics and classifiers [Martinek08] and NMF [You17]. You and others [You17] addressed detection using NMF for pattern modeling from the properties of the spectral structure of cough.
Classification of cough sounds is helpful in identifying the underlying cause or pathology so that appropriate treatment can be offered to patients. Most of the published work in this area performs manual detection of cough sounds before automatic classification can be performed. The main methods for classifying cough are based on energy thresholding [Chatrzarrin11], characteristics and classifiers [Infante17] [Amrulloh18] and wavelet [Kosasih15]. Chatrzarrin and others [Chatrzarrin11] found that the second phase of the dry cough has less energy compared to the wet cough. They also observed that, during this phase, most of the signal energy is contained between 0-750 Hz in the case of wet cough and 1500-2250 Hz in the case of dry cough. In [Kosasih15], they developed an algorithm for the automatic diagnosis of childhood pneumonia by evaluating the sounds of coughs and crackles. In the work [Amrulloh18], sound characteristics (MFCC, non-Gaussianity index, LPC and pitch) were extracted as input to a genetic algorithm to select the optimal characteristics and NN to classify wet and dry cough. Highlight the work [Cohen20] in which a database (NoCoCoDa) made up of cough sounds from subjects confirmed with COVID-19 is presented, including the annotation of the cough phases.
Some clinical works have reported that abnormal respiratory patterns could provide detailed clues for clinical treatments related to specific respiratory diseases [Boulding16], including novel analysis of the cadence associated to respiratory patterns of the breathing [Wang20]. On the other hand, wheezing sounds have been deeply investigated by the research team of this project [Torre18] [Torre19] [Torre20a] [Torre20b] [Torre20c] reaching competitive results in sound enhancement, detection, location and classification of this specific type of adventitious sounds. All commented works show the great interest, in recent years, of the scientific community in signal processing and AI in the biomedical field, including ECGs and biomedical sounds, and their possible applications in new areas of eHealth. One example of this effort is the detection of the presence of COVID-19. However, this is not the only application born under the eHealth paradigm. In the case of asthma disease, recently the following applications have been released for its individual management: i) Wheezo ( https://respiri.co/products/ ), an innovative eHealth platform to assist asthma patients with the management of their condition, especially children. Specifically, the device and eHealth app records and analyses breath sounds for the presence of wheezes in order to assist asthma monitoring; ii) Leo-sound ( https://hul.de/en/produkt/leosound-2/ ), a special developed new respiratory diagnostic system, that is able to record and analyze cough, breath and lung sounds over a long period; iii) WheezeScan ( https://www.omron-healthcare.co.uk/nebulisers/wheezescan.html ), a tool designed to detect wheeze in children with asthma symptoms.
In recent years, quantum machine learning (QML) has been proposed as a way of hybridizing techniques from classical machine learning and quantum computing. Although scalable and fault-tolerant quantum hardware is not yet available, some researchers have shown that quantum annealers like the ones offered by D-Wave can be used to obtain advantages over some classical methods in problems relevant to MINERVAS, like NMF factorization [O’Malley18][Golden20]. Also, some experiments with QML methods suggest that these techniques can obtain good classification results with less data than comparable classical machine learning methods [Mott17][Terashi20]. Moreover, in the case of the strong classifier constructed in [Mott17], the training on the quantum annealer is conducted off-line and the resulting model can be used afterwards on classical computers. It also leads to the possibility of interpreting the results since it implicitly selects the characteristics that are more relevant for the classification. This is helpful in reducing the number of features that need to be used. It is also important to notice that the quantum classifiers proposed, for instance, in [Hav19] and [Terashi20] use a reduced number of qubits so they can be efficiently simulated with classical computers and also lead to the development of quantum-inspired algorithms that can be run on classical hardware.
The consortium presented in the MINERVAS project has already begun to research in these fields, and they have a solid base in biomedical signal processing, time-frequency modeling, detection-classification, NMF techniques, machine learning, HPC techniques, quantum computing and software optimization in real-time on mobile devices, which guarantees the achievement of the objectives. This background has been acquired in previous projects, such as “Smart Sound Processing for the Digital Living” (TEC2015-67387) detailed above, in which both groups worked together.
Objectives
MINERVAS intends to demonstrate the usefulness and applicability of signal processing and AI techniques for monitoring biomedical information from the analysis of cardiac and pulmonary sound signals. The MINERVAS block diagram is shown in Figure 2.
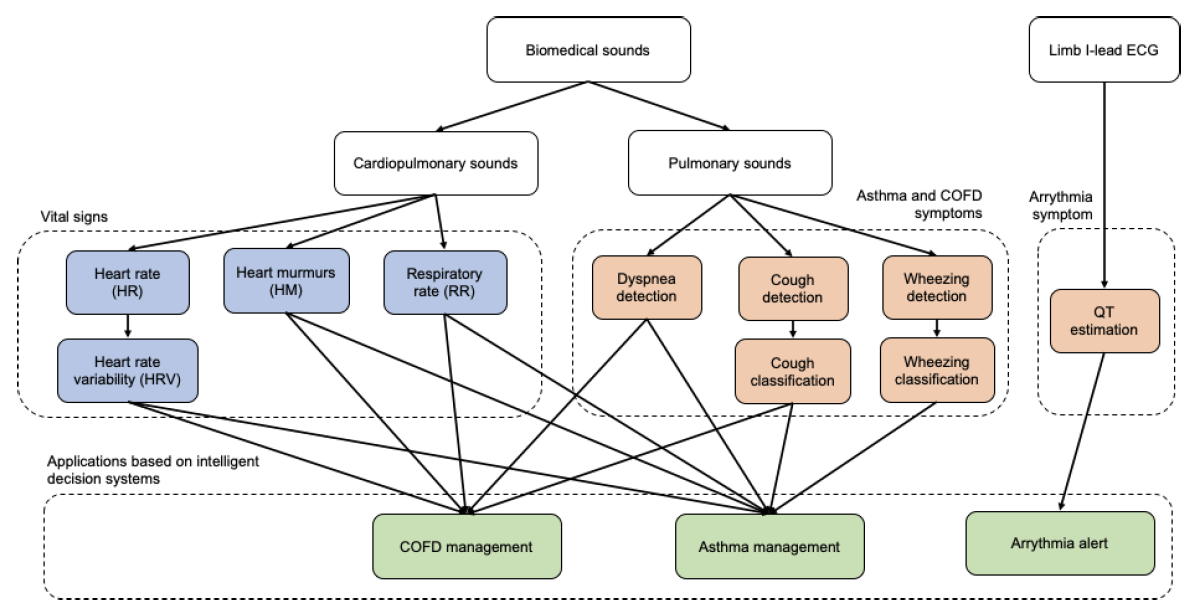 Figure 2. General outline of the proposed MINERVAS project.
Figure 2. General outline of the proposed MINERVAS project.Firstly, research and development of techniques for the estimation of cardiac vital signs (HR, QT) and respiratory (RR), as well as other biomedical parameters (HM and HRV) will be addressed. This approach makes it possible to improve the precision and reliability of the estimation of the above signs or to provide additional biomedical information useful to detect cardiac or respiratory disorders. Second, research and development of AI and signal processing techniques applied to the detection of sound events that commonly appear as symptoms of asthma and COPD, such as certain sounds of coughing, wheezing and respiratory dyspnea of the subject, will be addressed from sound signals captured by microphones. Finally, it is intended to implement systems in a mobile device to estimate the periods of exacerbation of asthma and COPD in the elderly and infants from the analysis of the sound signals of coughing and breathing.
Thus, according to MINERVAS hypothesis: i) From a medical point of view, the combination of the information from the estimation of HR, QT, HM, HRV, RR, cough, wheezing and respiratory dyspnea can accelerate the early detection of certain problems of health of the subject, which could lead to minimize medical decision times; ii) From the citizen's point of view, the development in portable devices of biomedical signal analysis applications can lead to the appearance of products with a highly beneficial impact on people's quality of life, especially in matters related to eHealth as it will allow individual monitoring of each person "anywhere", "at any time" (repetitiveness) and in an acceptable time, being available to practically "anyone", which could cause fewer citizens to visit health consultations in developed countries (reducing the probability of contagion for both the population and health personnel). Additionally, the proposed solution helps to give access to biomedical information to medical personnel with cheap equipment which is a key factor in countries with health systems with limited economic resources.
The hypothesis formulated will be demonstrated when the following general objectives are achieved:
- GO.1: AI and signal processing techniques for estimating biomedical information related to vital signs. The objective is to develop new reliable algorithms for signal processing and AI applied to the estimation of certain biomedical parameters, such as heart rate (HR), QT interval, heart murmurs (HM), heart rate variability (HRV) and respiratory rate (RR). We intend to estimate these parameters from the analysis of ECG signals and of sound signals from the auscultation process. The algorithms to be developed will focus on the detection of HR in cardiopulmonary sound sources, QT interval measurement for the sudden deaths risk estimation, detection of HM for the estimation of certain cardiac pathologies as well as for the improvement of HRV estimation in cardiopulmonary sound sources and RR detection from respiratory sound signals.
GO2: AI and signal processing techniques for estimating biomedical information related to cough and dyspnea. The goal is to develop new reliable AI and signal processing algorithms to detect and classify the different types of cough and to detect dyspnea. To do this, algorithms will be implemented to detect the presence of cough sound events and their subsequent classification to determine the degree of time-frequency similarity of sound pattern to different cough patterns. New AI and signal processing algorithms will also be developed for the detection of dyspnea in respiratory sounds (inhalation and exhalation through the mouth).
GO3: Design and implementation of intelligent applications for the automatic detection of pulmonary and/or cardiac alert situations. This project aims to develop intelligent systems in a mobile device for detecting the presence of alert situations from the analysis of cough and respiratory sound signals. It is very important to note that the development of these intelligent systems is based on the use of signal processing techniques and AI. Therefore, this device makes it possible to approach the concept of personalized medicine within the framework of a digitized society that offers continuous, non-invasive, reliable and low-cost monitoring through an application for mobile devices, devices available to the vast majority of the citizens. We intend to develop two different applications, one focused on asthma and other on COPD with the main goal of managing the elderly and nursling.
GO4: Design and implementation of an autonomous intelligent mobile application for the fatal ventricular arrhythmia risk level estimation. The objective is to have an autonomous application that allows the diagnostic automation of severe arrhythmia problems in patients with combined treatment, as a consequence of the prolongation of the QT interval, as is the case of the COVID-19 disease. This, in turn, will allow a significant reduction in reaction times to critical patient situations.Therefore, the application will offer the possibility of critical diagnosis in the normal situation of absence of specialized medical and/or nursing personnel. This application will be developed based on the QT interval evolution from the limb I-lead ECG, which is the available lead when using wearables, and some user’s clinical information. For this purpose, interpretable expert systems and knowledge acquisition systems will be used. As a consequence of the above, this project will prevent deaths due to the absence of diagnoses of fatal arrhythmias derived from the combined treatment, for instance.
Expected Results
The impact of the MINERVAS project is analyzed from five points of view:
1. Political impact. Our country belongs to the EU, one of the most developed regions in the world. MINERVAS proposes solutions and technologies to improve the quality of life not only in developed countries but also in countries with limited economic resources. The developed algorithms and value-added systems will improve comfort and well-being, generating knowledge with application to health and computational methodologies that could be exported to other application areas. These events will have a significant impact on the policy of the administrations, which should probably take into account the results of MINERVAS to define new services to improve the quality of life of citizens and minimize the costs of health systems.
2. Social impact. This project seeks the integration of personalized medicine in health care systems for the benefit of patients and citizens. Additionally, the needs of the most vulnerable groups thanks to both early detection of diseases and accelerate the decision times of the medical team.
In the field of health, the gender perspective refers to the need to recognize the differences between men and women, so that health outcomes and risks may be different. Until recently, public health, in the case of women, focused on pregnancy and childbirth, but a broader point of view is necessary, so that women's health is taken care of at all times. For example, cardiovascular disease affects many women, but this situation is often not recognized and diagnoses and treatments are delayed.
This proposal aims to contribute to the solution of technological problems oriented towards finding applications in the field of biomedicine considering cardiopulmonary sound signals relying, when necessary, on other types of vital signals and ECG data. Depending on the problem being addressed, the cardiopulmonary sounds may be nuanced by aspects related to body morphology, age (e.g. elderly and nursling), gender, etc. The metainformation of the data (of sounds and other vital signs) will be completed with attributes related to age and gender. In this project, the age and gender dimension is considered and it will be addressed in all the phases and the resulting applications will be adjusted to the particular needs.
3. Economic impact. By making use of ICTs, with companies in this technology sector involved such as 3M Littman (https://www.3m.com.es/3M/es_ES/Littmann-ES/) or Thinklabs (https://www.thinklabs.com/), a significant economic impact is expected, derived from the development of marketable applications and solutions. In this sense, the research generated can contribute to the economic development of two Autonomous Communities or the Country as a whole, generating employment in the R+D+i area. In addition, this consortium promotes the creation of new companies to take advantage of the results of the project.
4. Legal and sociological impact. There are some legal requirements that influence the expected impact from these points of view. Data protection must be taken into account, if sound databases and sensor data obtained from people are to be used. The people who participate in the generation of databases must be informed in advance that they are subject to such exercise and of the possible use of the data. Permission must be obtained from all of them, according to Directive 95/46 or EU, and the recent European Regulation for the Protection of Personal Data (RGPD). All these requirements will be addressed in the data management plan.
5. Impact on health. The monitoring of biological signals could have a significant impact from the point of view of health, maximizing the reliability of diagnoses and early detection with the acceleration in decision-making of medical teams. The knowledge generated in this project will be used by medical doctors through applications. This is the identification of the main contribution of the expected results to the selected challenge (Health).
Bibliographical references
[3m] 3M littmann stethoscopes. [Online]. Available: http://solutions.3m.com/ [Abaza09a] A. A. Abaza, A. M. Mahmoud, J. B. Day, W. T. Goldsmith, A. A. Afshari, J. S. Reynolds, and D. G. Frazer, Feature selection of voluntary cough patterns for detecting lung diseases, in 25th Southern Biomedical Engineering Conference, pp. 323–328, 2009[Alo13] P. Alonso, D. Argüelles, J. Ranilla, A.M. Vidal, A multicore solution to Block-Toeplitz linear systems of equations. Journal of Supercomputing, 65(3):999-1009, 2013.
[Alo17a] P. Alonso, P. Vera-Candeas, R. Cortina, J. Ranilla. An efficient musical accompaniment parallel system for mobile devices. Journal of Supercomputing, vol. 73, no. 1, pp. 343-353, 2017.
[Alo17b] P. Alonso, R. Cortina, F.J. Rodríguez-Serrano, P. Vera-Candeas, M. Alonso-González, J. Ranilla. Parallel online time warping for real-time audio-to-score alignment in multi-core systems. Journal of Supercomputing, vol. 73, no. 1, pp. 126-138, 2017
[Al-Khatib03] Al-Khatib SM, LaPointe NMA, Kramer JM, Califf RM. What Clinicians Should Know About the QT Interval. JAMA. 2003;289(16):2120–2127. doi:10.1001/jama.289.16.2120
[Amrulloh18] Y. Amrulloh, I. Priastomo, E. Wahyuni, and R. Triasih, Optimum Features Computation Using Genetic Algorithm for Wet and Dry Cough Classification, in Proceedings of 2018 2nd International Conference on Biomedical Engineering: Smart Technology for Better Society, IBIOMED, pp. 111-114, 2018
[Ari08] S. Ari, P. Kumar, G. Saha, A robust heart sound segmentation algorithm for commonly occurring heart valve diseases, J. Med. Eng. Technol., vol. 32, no. 6, pp. 456-465, 2008
[AudioSet] J. F. Gemmeke et al., Audio Set: An ontology and human-labeled dataset for audio events. 2017, Accessed: Jun. 19, 2020. [Online]. Available: https://research.google/pubs/pub45857/
[Bales20] C. Bales, M. Nabeel, C. John, U. Masood, H.Qureshi, H. Farooq, I. Posokhova and A. Can Machine Learning Be Used to Recognize and Diagnose Coughs?, arXiv, 2020
[Barry06] S. Barry, A. Dane, A. Morice, and A. Walmsley, The automatic recognition and counting of cough, Cough, vol. 2, no. 1, pp. 8-9, 2006.
[Ben11] P. Bentley, G. Nordehn, M. Coimbra and S. Mannor. The PASCAL Classifying Heart Sounds Challenge (CHSC2011) Results, Std., 2011. [Online]. Available: http://www.peterjbentley.com/heartchallenge/index.html
[Boelders2020] S. Boelders, V. Nallanthighal, V. Menkovski and A. Harma, Detection of mild dyspnea from pairs of speech recordings, ICASSP, 2020
[Boulding16] R.Boulding, R.Stacey, R.Niven, S.J.Fowler. Dysfunctional breathing: a review of the literature and proposal for classification, European Resp. Review, vol. 25, no. 141, pp. 287–294, 2016.
[Burgel2013] P. bulgel, J. Wedzicha, “Chronic cough in chronic obstructive pulmonary disease: time for listening?”. Am J Respir Crit Care Med ;187(9):902-4. 2013 May. DOI: 10.1164/rccm.201302-0332ED
[Cab14] P Cabañas-Molero, D Martínez-Muñoz, P Vera-Candeas, N Ruiz-Reyes, Voicing detection based on adaptive aperiodicity thresholding for speech enhancement in nonstationary noise. IET Signal Processing, vol. 8, no. 2, pp. 119-130, 2014.
[Cab18] P. Cabañas-Molero, P. Vera-Candeas, P. Alonso, J. Ranilla. Score identification based on audio-to-score alignment: complexity considerations. 18th Int. Conf. on Mathematical Methods in Science and Engineering (CMMSE 2018), Rota (Spain), July 2018.
[Cab19] P. Cabañas, R. Cortina, E. F. Combarro, P. Alonso, F.J. Bris. HReMAS: hybrid real-time musical alignment system. Journal of Supercomputing, vol. 75, no. 3, pp. 1001-1013, 2019.
[Canadas17] F.J. Canadas-Quesada, N. Ruiz-Reyes, J. Carabias-Orti, P. Vera-Candeas, J. Fuertes-Garcia, A non-negative matrix factorization approach based on spectro-temporal clustering to extract heart sounds, Applied Acoustics, vol. 125, pp. 7-19, 2017
[Cat17] T. Castro-de la Torre, N. Amador-Licona, E. Bernal-Ruíz, Correlation of heart rate variability with SYNTAX II on chronic angina. Rev Med Inst Mex Seguro Soc., vol. 55, 2017
[Chang20] S.Y. Chang, S. Vallecorsa, E.F. Combarro, F. Carminati. Quantum generative adversarial networks in a continuous-variable architecture to simulate high energy physics detectors. Machine Learning and the Physical Sciences Workshop at the 34th Conference on Neural Information Processing Systems (NeurIPS), 2020.
[Chatrzarrin11] H. Chatrzarrin, A. Arcelus, R. Goubran, F. Knoefel, Feature extraction for the differentiation of dry and wet cough sounds. IEEE International Workshop on Medical Measurements and Applications Proceedings (MeMeA), pp. 162-166, 2011
[Chatterjee12] Chatterjee H. K. Gupta R. Mitra M. Real time P and T wave detection from ECG using FPGA. Procedia Technology 4 (2012) 840-844 [Chen15] G. Chen, S. Imtiaz, E. Aguilar-Pelaez, E. Rodriguez-Villegas, Algorithm for heart rate extraction in a novel wearable acoustic sensor, Health Technol Lett., vol. 2, no. 1, pp. 28-33, 2015
[Chuah04] J. Chuah, Z. Moussavi, Automated respiratory phase detection by acoustical means, in Proc. 20th Annual Internat. Conf. Engineering in Medicine and Biology Society, pp. 21–24, 2004
[Cohen20] M. Cohen-McFarlane, R. Goubran and F. Knoefel, Novel Coronavirus Cough Database: NoCoCoDa, in IEEE Access, vol. 8, pp. 154087-154094, 2020
[Coc16a] A. Cocaña-Fernández, L. Sánchez, J. Ranilla. Improving the Eco-Efficiency of High Performance Computing Clusters Using EECluster. Energies, 9(197), 2016.
[Coc16b] A. Cocaña-Fernández, L. Sánchez, J. Ranilla. Leveraging a Predictive Model of the Workload for Intelligent Slot Allocation Schemes in Energy-Efficient HPC Clusters. Engineering Applications of Artificial Intelligence, 48: 95-105, 2016.
[Coc17] A. Cocaña, J. Ranilla, R. Gil, L. Sánchez. Multicriteria Design of Cost-Conscious Fuzzy Rule-Based Classifiers. Int. J. of Uncertainty, Fuzziness and Knowledge-Bases Systems, 25(Suppl 1): 141-159, 2017.
[Coc19a] A. Cocaña-Fernández, J. Rodríguez-Soares, L. Sánchez, J. Ranilla. Improving the energy efficiency of virtual data centers in an IT service provider through proactive fuzzy rules-based multicriteria decision making. Journal of Supercomputing, 15(3): 1078-1093, 2019.
[Coc19b] A. Cocaña-Fernández, E. San José Guiote E., L. Sánchez, J. Ranilla. Eco-Efficient Resource Management in HPC Clusters through Computer Intelligence Techniques. Energies, 12, 2129, 2019.
[Com19a] E.F. Combarro, I.F. Rúa, J. Ranilla. Experiments testing the commutativity of finite-dimensional algebras with a quantum adiabatic algorithm. Computational and Mathematical Methods in Science 1(1):e1009 (2019).
[Com19b] E.F. Combarro, J. Ranilla, I.F. Rúa. Quantum walks for the determination of commutativity of finite dimensional algebras. J. of Comp. and App. Math. 354:496-506 (2019).
[Com19c] E.F. Combarro, J. Ranilla, I.F. Rúa. A quantum algorithm for the commutativity of finite dimensional algebras. IEEE Access 7:45554-45562 (2019)
[Com20a] E.F. Combarro, J. Ranilla, I.F. Rúa. Quantum abstract detecting systems. Quantum Information Processing 19, 258 (2020)
[Com20b] E.F. Combarro, A. Piñera-Nicolás, J. Ranilla, I.F. Rúa. An explanation of the Bernstein-Vazirani and Deustch-Josza algorithms with the quantum stabilizer formalism. Computational and Mathematical Methods, in press (2020)
[Com20c] E.F. Combarro, F. Carminati, S. Vallecorsa, J. Ranilla, I.F. Rúa. On protocols for increasing the uniformity of random bits generated with noisy quantum computers. Journal of Supercomputing, accepted (2020)
[DCASE] A. Mesaros et al., Detection and Classification of Acoustic Scenes and Events: Outcome of the DCASE 2016 Challenge, IEEE/ACM Trans. Audio Speech Language Processing, vol. 26, no. 2, pp. 379–393, 2018
[Dia15] N. Díaz, A. Cocaña, M. Alonso, F.J. Martínez, R. Cortina, V.M. García, P. Alonso, J. Ranilla. Improving NNMFPACK with heterogeneous and efficient kernels for beta-divergence metrics. Journal of Supercomputing, 71(5): 1846-1856, 2015.
[Dia19] N.Dia, J.Fontecave-Jallon, P.Gumery, B.Rivet, Heart Rate Estimation from Phonocardiogram Signals Using Non-negative Matrix Factorization, IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, United Kingdom, pp. 1293-1297, 2019
[Doenges2020] Doenges, J., Kuckuck, E., Cassel, W. et al. “Disease control in patients with asthma and respiratory symptoms (wheezing, cough) during sleep”. Asthma Res. and Pract. 6, 9 (2020). https://doi.org/10.1186/s40733-020-00062-w
[El-Sherif-18] El-Sherif, N, Turitto, G, Boutjdir, M. Acquired long QT syndrome and torsade de pointes. Pacing Clin Electrophysiol. 2018; 41: 414– 421. https://doi.org/10.1111/pace.13296
[El-Sherif20] El-Sherif, N, Turitto G., Boutjdir M. (2020) Acquired Long QT Syndrome and Electrophysiology of Torsade de Pointes. In: El-Sherif N. (eds) Cardiac Repolarization. Springer, Cham. https://doi.org/10.1007/978-3-030-22672-5_11
[Fer20] M. Fernández-Pendás, E.F. Combarro, S. Vallecorsa, J. Ranilla, I.F. Rúa. A study of the performance of classical minimizers in the Quantum Approximate Optimization Algorithm. Journal of Computational and Applied Mathematics, accepted (2020)
[Ferdousi15]. B. Ferdousi, et al., Cough detection using speech analysis, 2015 18th International Conference on Computer and Information Technology (ICCIT), 2016
[Frappé2012] E. Frappé et al, “Chronic cough in the elderly is associated with expiratory flow limitation”. Rev Mal Respir;30(3):179-86, 2013 Mar. DOI: 10.1016/j.rmr.2012.09.020.
[Freesound] S. Music Technology Group at Universitat Pompeu Fabra, Barcelona, “freesound.” https://freesound.org/browse/.
[Garcia-Galan15] S. García-Galán, R.P. Prado, J.E. Muñoz-Expósito. Rules Discovery in Fuzzy Classifier Systems with PSO for Scheduling in Grid Computational Infrastructures. Applied Soft Computing, vol. 29, pp. 424-435, 2015. DOI: 10.1016/j.asoc.2014.11.064
[García-Galan20] Sebastián García-Galán, Mouad Seddiki, Rocio P. Prado, Jose Enrique Muñoz-Expósito, Adam Marchewka, and N. Ruiz-Reyes Relevance of Using Interpretability Indexes for the Design of Schedulers in Cloud Computing Systems IEEE World Congress on Computational Intelligence (WCCI) 2020. 19-24th July, 2020. Glasgow (UK), (2020)
[Ghaderi11] F. Ghaderi, H. Mohseni and S. Sanei, Localizing heart sounds in respiratory signals using singular spectrum analysis, IEEE Tran. on Biomed. Engineering, vol. 58, no. 12, pp. 3360-3367, 2011.
[Gil15] R. Gil, D. Ayllón, J. Ranilla, C. LLerena, I. Diaz. A Computationally Efficient Sound Environment Classifier for Hearing Aids. IEEE Trans. Biom. Eng., 62(10): 2358-2368, 2015.
[Gil17] R. Gil, J. García, M. Bautista, E.F. Combarro, A. Cocaña. Evolved frequency log-energy coefficients for voice activity detection in hearing aids. 2017 IEEE Int. Conf. on Fuzzy Systems (FUZZ-IEEE 2017), Naples (Italy), July 2017.
[Golabbakhsh05] M. Golabbakhsh, Z. Moussavi and M. Aboofazeli, Respiratory flow estimation from tracheal sound by adaptive filters, Proc IEEE Annual Conference Engineering in Medicine and Biology, vol. 4, pp. 4216-4219, 2005
[Golden20] J. Golden and D. O'Malley. Reverse Annealing for Nonnegative/Binary Matrix Factorization. arXiv preprint arXiv:2007.05565 (2020).
[Gomes18] L. Gomes, N. Oliveira, L. Tauil, R. Mattos and P. Melo, Instrumentation for respiratory flow estimation using tracheal sounds analysis: Design and evaluation in measurements of respiratory cycle periods and airflow amplitude, Journal of Physics Conference Series, vol. 1044, no. 1, 2018
[H2020bio] Health, demographic change and wellbeing, Work Programme 2018-2020, Horizon 2020, https://ec.europa.eu/research/participants/data/ref/h2020/wp/2018-2020/main/h2020-wp1820-health_e n.pdf
[GRDC] Chronic Respiratory Disease Collaborators. “Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017”. The Lancet. Vol. 8, no. 6, pp 585-596, June 01, 2020.
[Guenter18] K. Guenter, W. Cassel, O. Hildebrandt, J. Kroenig, P. Fische, A. Weissflog, C. Vogelmeier, U. Koehler, Control of Respiratory Symptoms During Sleep in Patients with Stable Bronchial Asthma, Dtsch Med Wochenschr, vol. 143, no. 18, 2018, doi: 10.1055/a-0623-865 1
[Haixia19] Haixia Shang, Shoushui Wei, Feifei Liu, Dingwen Wei, Lei Chen,and Chengyu Liu. “AnImproved Sliding Window Area Method for T-Wave Detection”. Hindawi Computational andMathematical Methods in Medicine Volume 2019, Article ID 3130527, 11 pages
[Hav20] Havlíček, V., Córcoles, A. D., Temme, et al. Supervised learning with quantum-enhanced feature spaces. Nature, 567(7747), 209-212, 2019
[Hillman05] K. Hillman, J. Chen, M. Cretikos, R. Bellomo, D. Brown et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial, vol. 365, pp. 2091–2097, Lancet, 2005
[Hult00] P. Hult, B. Wranne, and P. Ask, A bioacoustic method for timing of the different phases of the breathing cycle and monitoring of breathing frequency, Medical Engineering Physics, vol. 22, no. 6, pp. 425–433, 2000
[ICBHI] ICBHI 2017 Challenge. [Online]. Available: https://bhichallenge.med.auth.gr/sites/default/
[Immanuel16] S.A.Immanuel, A.Sadrieh, M.Baumert et al, T-wave morphology can distinguish healthy controls from LQTS patients, Physiological Measurement, vol. 37, no. 9, pp. 1456–1473, 2016
[Infante17] C. Infante, D. Chamberlain, R. Fletcher, Y. Thorat and R. Kodgule, Use of cough sounds for diagnosis and screening of pulmonary disease, IEEE global humanitarian technology conference. GHTC), p. 1–10, 2017.
[Jankelson20] Jankelson L, Karam G, Becker ML, Chinitz LA, Tsai MC. QT prolongation, torsades de pointes, and sudden death with short courses of chloroquine or hydroxychloroquine as used in COVID-19: A systematic review. Heart Rhythm . 2020; 17(9): 1472-1479. doi:10.1016/j.hrthm.2020.05.008
[Jusak16] J. Jusak, I. Puspasari and P. Susanto, Heart murmurs extraction using the complete Ensemble Empirical Mode Decomposition and the Pearson distance metric, International Conference on Information & Communication Technology and Systems (ICTS), pp. 140-145, 2016
[Kamran13] H. Kamran, I. Naggar, F. Oniyuke, M. Palomeque, P. Chokshi, L. Salciccioli, M. Stewart, and J. M. Lazar, Determination of heart rate variability with an electronic stethoscope, Clinical automatic research, vol. 23, pp. 41-47, 2013.
[Kellet11] J. Kellett, M. Li, S. Rasool, G. Green and A. Seely, Comparison of the heart and breathing rate of acutely ill medical patients recorded by nursing staff with those measured over 5 min by a piezoelectric belt and ECG monitor at the time of admission to hospital, Resuscitation, vol. 82, pp. 1381-1386, 2011
[Kelly19] Kelly, et al. Key challenges for delivering clinical impact with artificial intelligence. BMC Med 17, 195 (2019). https://doi.org/10.1186/s12916-019-1426-2.
[Kosasih15] K. Kosasih et al., Wavelet augmented cough analysis for rapid childhood pneumonia dIagnosis, IEEE Transactions on Biomedical Engineering, vol. 62, no. 4, pp. 1185-1194, 2015
[Kulkas09] A. Kulkas, E. Huupponen, J. Virkkala, M. Tenhunen, A. Saastamoinen, E. Rauhala, and S. Himanen, Intelligent methods for identifying respiratory cycle phases from tracheal sound signal during sleep, Computers in Biology and Medicine, vol. 39, no. 11, pp. 1000–1005, 2009.
[Kumar06] D. Kumar, P. Carvalho, M. Antunes, P. Gil, J. Henriques and L. Eugenio, A new algorithm for detection of S1 and S2 heart sounds, IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Toulouse, France, 2006
[Latif20] S. Latif, M. Usman, S. Manzoor, W. Iqbal, J. Qadir, G. Tyson, I. Castro, A. Razi, M. N. K. Boulos, A.Weller et al., Leveraging data science to combat covid-19: A comprehensive review, IEEE Transactions on Artificial Intelligence, 2020. DOI: 10.1109/TAI.2020.3020521
[Li13] T. Li, A Heart Sound Segmentation Method Based on Cyclostationary Envelope, Proc. of the 2nd International Conference on Computer Science and Electronics Engineering (ICCSEE), 2013
[Lippincott] Lippincott Nursing Center. [Online]. Available: https://www.nursingcenter.com/ .
[Lop16b] M. Lopez-Portugues, J.A. Lopez-Fernandez, J. Ranilla, R.G. Ayestaran, F. Las-Heras. Using heterogeneous computing for scattering prediction in scenarios with several source configurations. Journal of Supercomputing 73(1):57-74, 2017
[Liu19] H. Liu, J. Allen, D. Zheng and F. Chen, Recent development of respiratory rate measurement technologies, Physiology Measurement, vol. 40, no. 7, 2019
[Lu16] B. Lu, Unidirectional Microphone based Wireless Recorder for the Respiration Sound, Journal of Bioengineering & Biomedical Science, vol. 6, no. 3, 2016
[Martinek08] J. Martinek, M. Tatar, M. Javorka, Distinction between voluntary cough sound and speech in volunteers by spectral and complexity analysis., Journal of Physiology and Pharmacology, vol. 59, no. 6, pp. 433-440, 2008
[Matos07] S. Matos, S. Birring, I. Pavord and et al., An automated system for 24 h monitoring of cough frequency: the Leicester cough monitor, IEEE Transactions on Biomedical Engineering, vol. 54, no. 8, pp. 1472-1478, 2007
[Mott17] Mott, A., Job, J., Vlimant, J. R., Lidar, D., and Spiropulu, M. Solving a Higgs optimization problem with quantum annealing for machine learning. Nature, 550(7676), 375-379, 2017.
[Muñ18] P. Muñoz, F.J. Bris, P. Alonso, J. Ranilla. Online score-informed source separation in polyphonic mixtures using instrument spectral patterns. 18th Int. Conf. on Mathematical Methods in Science and Engineering, Rota (Spain), July 2018.
[Muñ19] Muñoz-Montoro, A.J., Ranilla, J., Vera-Candeas, P., Combarro, E.F., Alonso-Jordá, P. Real-time Soundprism. Journal of Supercomputing, vol. 75, no. 3, pp. 1594-1609, 2019.
[Muñ20a] Muñoz-Montoro, A.J., Cortina, R., García-Galán, S., Combarro, E.F., Ranilla, J. A score identification parallel system based on audio-to-score alignment. Journal of Supercomputing, vol. 76, pp, 8830-884, 2020.
[Muñ20b] Muñoz-Montoro, A.J., Suarez-Dou, D., Cortina, R., Canadas-Quesada, F.J., Combarro. Parallel source separation system for heart and lung sounds. Journal of Supercomputing, accepted.
[Muthusamy19] P. Muthusamy, K. Sundaraj, N. Manap, An Overview of Respiratory Airflow Estimation Techniques: Acoustic vs Non-Acoustic, IEEE International Conference on Signal and Image Processing Applications (ICSIPA), pp. 149-153, 2019
[Nakano04] H. Nakano, M. Hayashi, E. Ohshima, N. Nishikata, and T. Shinohara, Validation of a new system of tracheal sound analysis for the diagnosis of sleep apnea-hypopnea syndrome, Sleep, vol. 27, no. 5, pp. 951-958, 2004.
[Nallanthighal2020] V. Nallanthighal, A. Harma, and H. Strik, Speech breathing estimation using deep learning methods, IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), pp. 1140-1144, 2020
[Nallanthighal19] V. Nallanthighal, A. Harma, and H. Strik, Deep Sensing of Breathing Signal During Conversational Speech, in Interspeech, pp. 4110-4114, 2019
[Nam2016] Y. Nam, Y. Kong, B. Reyes, N. Reljin and K. Chon, Monitoring of Heart and Breathing Rates Using Dual Cameras on a Smartphone. PloS one, vol. 11, no. 3, 2016
[Nam2016a] Y. Nam, B. Reyes and K. H. Chon, Estimation of Respiratory Rates Using the Built-in Microphone of a Smartphone or Headset, in IEEE Journal of Biomedical and Health Informatics, vol. 20, no. 6, pp. 1493-1501, 2016
[Naseri13] H. Naseri and M. Homaeinezhad, Detection and Boundary Identification of Phonocardiogram Sounds Using an Expert Frequency- Energy Based Metric, Annals of Biomedical Engineering, vol. 41, pp. 279-292, 2013
[Niimi2011] A. Niimi, “Cough and Asthma”, Curr Respir Med Rev.; 7(1): 47–54. 2011 Feb. DOI: 10.2174/157339811794109327.
[Noisex90] Signal Processing Information Base (SPIB). NOISEX database. Speech 618 Babble, http://spib.linse.ufsc.br/noise.html, Online. Accessed: 2020-04-27 (1990).
[Oletic17] D. Oletic and V. Bilas, Asthmatic wheeze detection from compressively sensed respiratory sound spectra, IEEE Journal of Biomedical and Health Informatics, 2017
[O’Malley18] D. O’Malley, V.V., Vesselinov, B.S. Alexandrov and L.B. Alexandrov. Nonnegative/binary matrix factorization with a d-wave quantum annealer. PloS one , 13 (12), 2018.
[OMSa] Organización Mundial de la Salud. Enfermedades cardiovasculares. https://www.who.int/cardiovascular_diseases/about_cvd/es/
[OMSb] Organización Mundial de la Salud. Enfermedades respiratorias crónicas. https://www.who.int/respiratory/es/
[OMSc] World Health Organization, “Coronavirus disease (COVID-19) outbreak situation,” WHO, 2020. https://www.who.int/emergencies/diseases/novel- coronavirus-2019
[Ort20] F. Orts, G. Ortega, E. F. Combarro, E. Garzón. A review on reversible quantum adders. Journal of Network and Computer Applications, in press (2020)
[Pal13] R. Palaniappan, K. Sundaraj and N. Ahamed, Machine learning in lung sound analysis: A systematic review, Biocybernetics and Biomedical Engineering, vol. 33, no. 3, pp. 129-135, 2013
[Palaniappan15] R. Palaniappan, K. Sundaraj, and F. Nabi, An Overview of Breath Phase Detection – Techniques & Applications, Journal of Telecommunication, Electronic and Computer Engineering, vol. 10, no. 2-7, pp. 33-36, 2015
[Papadaniil14] C. Papadaniil and L. Hadjileontiadis, Efficient heart sound segmentation and extraction using ensemble empirical mode decomposition and kurtosis features,” IEEE Journal of Biomedical and Health Informatics., vol. 18, no. 4, pp. 1138-1152, 2014
[Physionet06] PhysioNet/Computers in Cardiology Challenge QT Interval Measurement. 2006. http://www.physionet.org/challenge/2006/
[Physionet16] PhysioNet/CinC challenge. National Institute of General Medical Sciences and the National Institute of Biomedical Imaging and Bioengineering, https://www.physionet.org/physiobank/database/challenge/2016/, 2013, Online.
[Rahul20] Rahul, J., Sora, M. & Sharma, L.D. Exploratory data analysis based efficient QRS-complex detection technique with minimal computational load. Phys Eng Sci Med 43, 1049–1067 (2020). https://doi.org/10.1007/s13246-020-00906-y
[Rale] The r.a.l.e. repository. [Online]. Available: http://www.rale.ca/
[RCP15] The ABCDE Approach, Resuscitation Council UK, 2015. https://www.resus.org.uk/library/2015-resuscitation-guidelines/abcde-approach
[RCP17] National Early Warning Score (NEWS) 2, Royal College of Physicians, 2020. https://www.rcplondon.ac.uk/projects/outputs/national-early-warning-score-news-2
[Rodriguez19] R. Rodríguez-Reche, R.P. Prado, S. García-Galán, J.E. Muñoz-Expósito, N. Ruiz-Reyes. Specific Parameter-Free Global Optimization to Speed up Setting and Avoid Factors Interactions. Computing and Informatics. Vol. 38, Nº2. pp:265-290. 2019. DOI: 10.31577/cai_2019_2_265
[Roversi2018] S. Roversi et al, “Breathlessness, but not cough, suggests chronic obstructive pulmonary disease in elderly smokers with stable heart failure”, Multidiscip Respir Med 13, 35 (2018). https://doi.org/10.1186/s40248-018-0148-1
[Schuller20a] B. Schuller, D. Schuller, K. Qian, J. Liu, H. Zheng and X. Li, COVID-19 and Computer Audition: An Overview on What Speech & Sound Analysis Could Contribute in the SARS-CoV-2 Corona Crisis, arXiv, 2020
[Schuller20b] B. Schuller, A. Batliner, C. Bergler, E. Messner, A. Hamilton, S. Amiriparian, A. Baird, G. Rizos, M. Schmitt, L. Stappen, H. Baumeister, A. D. MacIntyre, and S. Hantke, The INTERSPEECH 2020 Computational Paralinguistics Challenge: Elderly Emotion, Breathing & Masks, in Proceedings Interspeech, Shanghai, China, 2020
[Ses18] F. Sessa, V. Anna, G. Messina, G. Cibelli, V. Monda, G. Marsala, M. Salerno, Heart rate variability as a predictive factor for sudden cardiac death. Aging, vol. 10, no. 2, pp. 166-177, 2018.
[Shah14] G. Shah, P. Koch and C. Papadias, Analysis of Acoustic Cardiac Signals for Heart Rate Variability and Murmur Detection Using Nonnegative Matrix Factorization-Based Hierarchical Decomposition, IEEE Int. Conf. on Bioinformatics and Bioengineering, pp. 46-53, 2014
[Sharma14] P. Sharma, S. Saha and S. Kumari, Study and Design of a Shannon- Energy-Envelope based Phonocardiogram Peak Spacing Analysis for Estimating Arrhythmic Heart-Beat, International Journal of Scientific and Research Publications, vol. 4, no. 9, september, 2014
[Sharma19] P. Sharma and E. Rodriguez-Villegas, A Novel Algorithm for HRV Estimation from Short-Term Acoustic Recordings at Neck, 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, pp. 6343-6346, 2019
[Shi20] L. Shi, Y. Wang, Y. Wang, G. Duan and H. Yang, Dyspnea rather than fever is a risk factor for predicting mortality in patients with COVID-19, The Journal of infection, vol. 81, no. 4, pp. 647-679, 2020
[Smith2006] J. Smith, A. Woodcock, “Cough and its importance in COPD”. Int J Chron Obstruct Pulmon Dis; 1(3): 305–314; 2006 Sep. DOI: 10.2147/copd.2006.1.3.305
[Spadaccini15] A. Spadaccini and F. Beritelli, Performance evaluation of heart sounds biometric systems on an open dataset, 18th International conference on digital signal processing (DSP), Fira, Greece, 2013
[Spring15] Spring DPTE 516 medical issues I – lung sounds, University of Maryland, Baltimore. [accessed: 2015-10-15]. https://itunes.apple.com/us/itunes-u/spring-dpte-516-medicalissues/id431166351?mt=10
[Srikanth19] V. Nallanthighal, A. Harma and H. Strik, Deep Sensing of Breathing Signal During Conversational Speech, in Interspeech, pp. 4110-4114, 2019
[Sumner2013] H. Sumner et al, “Predictors of objective cough frequency in chronic obstructive pulmonary disease”. Am J Respir Crit Care Med. 187(9):943-9, 2013 May. DOI: 10.1164/rccm.201211-2000OC.
[Stetho] Stethographics lung sound samples. [Online]. Available: http://www.stethographics.com/
[Targeted] R. Pramono, S. Imtiaz, and E. Rodriguez- Villegas, A Cough-Based Algorithm for Automatic Diagnosis of Pertussis, PLoS ONE, vol. 11, no. 9, 2016
[Tennessee] East tennessee state university pulmonary breath sounds. [Online]. Available: http://faculty.etsu.edu .
[Terashi20] Terashi, K., Kaneda, M., Kishimoto, T., Saito, M., Sawada, R., and Tanaka, J.. Event Classification with Quantum Machine Learning in High-Energy Physics. arXiv preprint arXiv:2002.09935, 2020
[Timit] J. Garofolo et al., TIMIT: Acoustic-phonetic Continuous Speech Corpus. Linguistic Data Consortium, Philadelphia, 1993
[Torre18] J Torre-Cruz, F Canadas-Quesada, P Vera-Candeas, V Montiel-Zafra, N Ruiz-Reyes, Wheezing sound separation based on constrained non-negative matrix factorization, Proceedings of the 2018 10th International Conference on Bioinformatics and Biomedical Technology, pp. 18-24, 2018 ACM Conference Proceedings (ISBN: 978-1-4503-6366-2), Best Oral Presentation Award
[Torre19] J. Torre-Cruz, F. Canadas-Quesada, J. Carabias-Orti, P. Vera-Candeas, N. Ruiz-Reyes, A novel wheezing detection approach based on constrained non-negative matrix factorization, Applied Acoustics, vol. 148, pp. 276-288, 2019
[Torre20a] J. Torre-Cruz, F.J. Cañadas-Quesada, N. Ruiz-Reyes, P. Vera-Candeas and J.J. Carabias-Orti, Wheezing Sound Separation Based on Informed Inter-Segment Non-Negative Matrix Partial Co-Factorization, Sensors, vol. 20, no. 9, 2020
[Torre20b] J. Torre-Cruz, F.J. Cañadas-Quesada, J.J. Carabias-Orti, P. Vera-Candeas, N. Ruiz-Reyes, Combining a recursive approach via non-negative matrix factorization and Gini index sparsity to improve reliable detection of wheezing sounds, Expert Systems with Applications, vol. 147, 2020
[Torre20c] J. Torre-Cruz, F. Canadas-Quesada, S. García-Galán, N. Ruiz-Reyes, P. Vera-Candeas, J. Carabias-Orti, A constrained tonal semi-supervised non-negative matrix factorization to classify presence/absence of wheezing in respiratory sounds, Applied Acoustics, vol. 161, pp. 2020
[Torre20d] J. Torre-Cruz, F. Canadas-Quesada, D. Martiınez, N. Ruiz, S. García-Galán, J. Carabias, An incremental algorithm based on multichannel non-negative matrix partial co-factorization for ambient denoising in auscultation, Applied Acoustics, 2020, Status: Under Review.
[TUT17a] TUT Sound events 2017, Development dataset, https://zenodo.org/record/814831, Online. Accessed: 2020-04-27 (2017).
[TUT17b] TUT Sound events 2017, Evaluation dataset, https://zenodo.org/record/1040179, Online. Accessed: 2020-04-27 (2017).
[Ulukaya19] S. Ulukaya, G. Serbes, Y. P. Kahya, Wheeze type classification using non-dyadic wavelet transform based optimal energy ratio technique, Computers in biology and medicine vol. 104, pp. 175-182, 2019.
[Wang20] Y. Wang, M. Hu, Q. Li, X.-P. Zhang, G. Zhai, and N. Yao, Abnormal respiratory patterns classifier may contribute to large-scale screening of people infected with covid-19 in an accurate and unobtrusive manner, arXiv, 2020.
[Wei19] W. Wei, G. Zhan, X. Wang, P. Zhang and Y. Yan, A Novel Method for Automatic Heart Murmur Diagnosis Using Phonocardiogram, International Conference on Artificial Intelligence and Advanced Manufacturing (AIAM), 2019
[Weinberger2007] M. Weinberger, M. Abu-Hasan, “Pseudo-asthma: When Cough, Wheezing, and Dyspnea Are Not Asthma”. Pediatrics, 120 (4) 855-864, October 2007; DOI: https://doi.org/10.1542/peds.2007-0078.
[Yadollahi06] A. Yadollahi and Z. M. Moussavi, A robust method for estimating respiratory flow using tracheal sounds entropy,” IEEE Transactions on Biomedical Engineering, vol. 53, no. 4, pp. 662-668, 2006
[Yil14] M. Yıldız and Z. Türkoğlu, Feasibility of heart rate variability analysis with heart sounds, 22nd Signal Processing and Communications Applications Conference (SIU), 2014
[You17] M. You, H. Wang, Z. Liu, C. Chen, J. Liu, X. Xu, Z. Qiu, Novel feature extraction method for cough detection using NMF, IET Signal Processing, vol. 11, no. 5, pp. 515-520, 2017
[Yuenyong11] S. Yuenyong, A. Nishihara, W. Kongprawechnon and K. Tungpimolrut, A framework for automatic heart sound analysis with segmentation, Biomedical Engineering Online, vol. 10, no. 13, 2011.